Asthma Disparities and Health Inequities
What are health disparities?
Health disparities occur when there is a difference in health outcomes between populations. Healthy People 2020 has defined health disparities as “a particular type of health difference that is closely linked with social, economic, and/or environmental disadvantage. Health disparities adversely affect groups of people who have systematically experienced greater obstacles to health based on their racial or ethnic group; religion; socioeconomic status; gender; age; mental health; cognitive, sensory, or physical disability; sexual orientation or gender identity; geographic location; or other characteristics historically linked to discrimination or exclusion” 1. Both the Centers for Disease Control and Prevention and Healthy People 2020 have prioritized promoting health equity and reducing health disparities.
What is health equity?
Health equity can be described as “the state in which everyone has the opportunity to attain full health potential and no one is disadvantaged from achieving this potential because of social position or any other socially defined circumstance” 2. When considering a person’s health there are things people cannot control such as genetics and biology. Achieving health equity involves addressing the modifiable factors affecting the health of individuals and communities. Health disparities are often contributing factors that make achieving health equity more challenging. Factors that contribute to both health equity and health disparity are referred to as the “social determinants of health”.





Social determinants of health (SDOH) is a broad term describing “conditions in the environments in which people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks” 3. These factors include socioeconomic status, education, the neighborhoods and physical environments in which people live, employment opportunities, social support, and access to health care 4. These factors can impact the physical and mental health of individuals, as well as their ability to manage chronic conditions.
Access to quality educational and employment opportunities, physically and environmentally safe neighborhoods, ability to afford and obtain food, access to culturally competent health care, and social support systems are all crucial to health. Without access to quality education, people may be less likely to obtain steady employment with a decent income and access to health insurance. This may contribute to affording safe (both physically and environmentally) housing and the ability to afford and access healthy foods. People may have to choose between food and housing over getting medical care and medications. Unfortunately, the emergence of COVID-19 has highlighted how social determinants of health are a major issue adversely affecting many populations.
“Maybe this is the year we finally got serious about addressing health disparities”
Jerome Adams, MD, MPH
Vice Admiral, US Public Health Service
Surgeon General of the United States
When considering asthma and allergies, these are both conditions that require ongoing care and maintenance to maintain adequate control. Medication compliance is important to manage both asthma and allergies, but people may not use medications as directed or may ration them if they can’t afford the cost. This occurs with maintenance medications such as inhalers or rescue medications like quick-relief inhalers and epinephrine auto-injectors. Finances, as well as limited or no transportation may also cause patients to delay or forgo follow-up with their doctors. Some people may also live in an area where a lung doctor or allergist may not be readily available. Urban environments may have substandard housing with more exposure to asthma and allergy triggers such as mold, dust mites, mice, cockroaches, and pollution. Cultural and language barriers can also play a role in understanding health information, such as how to use an inhaler correctly. Even access to allergen-free food may be a barrier for patients due to cost or just lack of options for obtaining groceries.

What is health literacy?
Health literacy is “the degree to which an individual has the capacity to obtain, communicate, process, and understand basic health information and services to make appropriate health decisions” 30.
Literacy (the ability to read or write) does not mean a person has good health literacy. Health literacy goes beyond the ability to read or write to reflect an understanding of basic health information as described above.

How is health literacy linked to health disparities?
Individuals living with health disparities are more likely to have lower levels of health literacy.
Low health literacy is more common in older adults, minority populations, people with low socioeconomic status, and those who are medically underserved 30.

How does health literacy impact people with asthma and allergies?
Health literacy is an important part of managing chronic health conditions, such as asthma and allergies.
Lower health literacy can lead to poor control of any chronic conditions. It can also lead to severe consequences. For example, if a person can’t read and understand a medication label, they could accidentally overdose on a medication, which could be fatal.
People with lower health literacy may also need extra education on their conditions in simple, easy to understand language. They may also need assistance navigating the health care system, including finding resources and providers. It is also important that patients see culturally competent providers, including providers that speak their language and may understand cultural norms and barriers to achieving health.
Download “Disparities in Asthma: Who’s at Risk?” PDF

How do health disparities affect African Americans?
In 2017, there were 41.4 million African Americans living in the U.S., representing 12.7% of the total population 5. Across the board, African Americans have lower life expectancy than whites 5. Conditions such as hypertension, obesity, asthma, and diabetes are more prevalent in African Americans 6,7,8,9. Historically, the African American community distrusts the medical community, and public health guidance, and they are often hesitant to engage in clinical research 28.
African Americans are the second largest minority population in the U.S., behind Hispanics 5. Most (58%) African Americans live in the southern U.S. 5. Compared to non-Hispanic whites, African Americans have lower rates of educational attainment from high school graduation through graduate degrees 5. The median household income is $40,165 compared to $65,845 in non-Hispanic whites 5. African Americans have higher rates of poverty with 22.9% of households living in poverty, which is over double the percent of non-Hispanic white households 5. They also have over double the rates of unemployment, at 9.6 percent 5. Nearly 10% of African Americans are uninsured 5. Life expectancy for African Americans is lower for both men and women 5. Of the 10 counties in the U.S. with the highest rates of food insecurity, 9 are in the south 12. Of these 10 counties, at least 60% of the population is African American 13. Over 21 percent of African American households are food insecure across the U.S. 14. African Americans are also more likely than non-Hispanic whites to live near facilities releasing air pollutants 15. African American renters spend a larger portion of their income on rent than white renters 16 and account for 40 percent of those experiencing homelessness 17.
How do health disparities affect Hispanics?
There are 58.8 million Hispanics in the U.S., representing 18.1% of the population 18. Hispanics have the same prevalence of hypertension as non-Hispanic whites 6. Hispanics have the second highest rate of obesity, below African Americans, but above non-Hispanic whites 7. Hispanics have lower rates of asthma than both African Americans and non-Hispanic whites (with the exception being Puerto Ricans who have nearly double the incidence of asthma) 8,19. Hispanics have higher rates of diabetes than non-Hispanic whites 9. Hispanics have lower rates of heart disease non-Hispanic whites 10. Another feature of the Hispanic population in the U.S. is that it is young. One third of Hispanics are under the age of 18 and nearly 60% are millennials, or younger, which may play a role in the rates of chronic disease prevalence 20.
Over 70% of Hispanics speak a language other than English at home, with nearly 30% reporting that they are not fluent in English 18. This can be a barrier to accessing health care, finding culturally competent health care providers, and understanding health information. Less than 70% of Hispanics have a high school diploma and fewer than 16% have a bachelor’s degree or higher 18. The average household income in Hispanic families is $49,793, with unemployment at 6% and poverty levels of 19.4% 18. Affording healthcare is significant issue within the Hispanic community as they have the highest number of uninsured people at 17.8% 18. While nationally, 13.9% of households lack regular access to foods that support an active life and healthy diet, that number is higher in Hispanics at 16.2% 14.
How do health disparities affect American Indians and Alaskan Natives?
There are 5.6 million American Indians and Alaskan Natives living in the U.S, which is 1.7% of the total population 21. American Indians and Alaskan Natives have higher rates of hypertension, obesity, asthma, and heart disease than non-Hispanic whites 22. American Indians and Alaskan Natives also have the highest rates of diabetes amongst all racial and ethnic groups in the U.S. 23.
There are several disparities in the social determinants of health for American Indians and Alaskan Natives. While 22% of the population lives on reservations or trust lands, another 60% live in metropolitan areas, but that is lower than any other racial or ethnic population in the U.S.21. American Indians and Alaskan Natives have lower rates of educational attainment from high school through graduate degrees that non-Hispanic whites 21. The average household income is $45,448 and 21.9% of households live in poverty 21. The percent of American Indians and Alaskan Natives without health insurance is 14.9%. Nearly 25% of households lack regular access to foods that support an active life and healthy diet 24. Specific to the Navajo Nation, 30-40% of residents do not have running water and the nation is considered a “food desert” (meaning access to affordable and healthy food is severely limited) 25.


Quick 3-5 minute videos on asthma, allergies, and related conditions.
How are health disparities a factor in the era of COVID-19?
While the issue of health disparities is nothing new, the emergence of COVID-19 has shed a spotlight on them as the virus has been particularly devastating to communities of color. Nearly 90% of those hospitalized with COVID-19 have underlying medical conditions, including hypertension, obesity, chronic lung disease, diabetes, and heart disease 26, many of which disproportionately affect African Americans, Hispanics, and American Indians or Alaskan Natives.
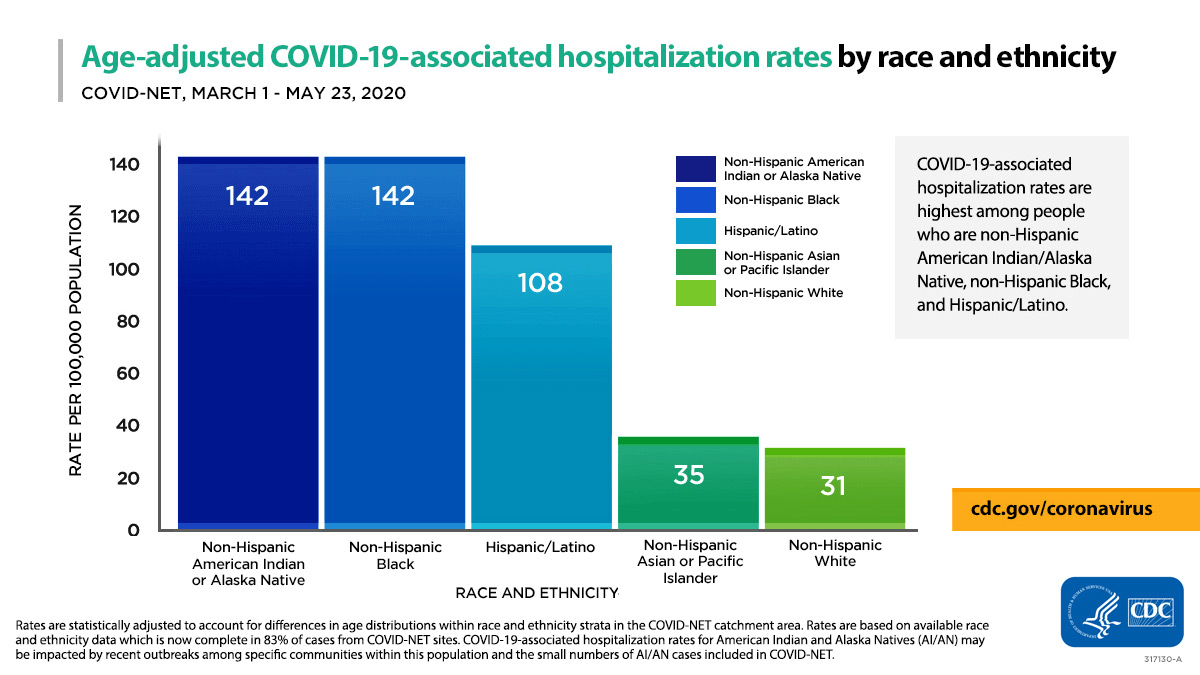
Racial and ethnic information is only available for about 35% of the deaths across the U.S. 11,26. In states reporting racial and ethnic data, African Americans make up 13% of the population, but account for 34% of deaths 11. African Americans are tied with American Indians and Alaskan Natives for the highest hospitalization rate at 142 per 100,000 28. Hispanics remain disproportionately affected in terms of hospitalization rates from COVID-19, with the third highest of any ethnic group, at 108 hospitalizations per 100,000 people 28.

In many states with higher percentages of Hispanics, they make up for a higher percent of cases. Interestingly, however, outside of New York, they do not have a disproportionate number of deaths 29, which may have something to do with the Hispanic population being generally younger and having fewer health disparities. The Navajo Nation now has the highest, per capita, rates of COVID-19 in the U.S. 25. Understanding the racial and ethnic impact of COVID-19 is somewhat limited as not all states are not reporting data on cases and deaths by race or ethnicity 11.

Why is it important to have diversity in research?
Conducting research with a diverse patient population is important as it reflects the broad population and helps identify issues that may affect certain patients differently than others. However, the under representation of minority populations in clinical research is an ongoing challenge that makes it difficult to generalize findings 31. In research funded by the National Institutes of Health, between 1993 and 2013, the inclusion of racial or ethnic minorities was reported in less than 5% of research on respiratory diseases 32.
Involving diverse patients in all phases of research provides insights into the target population 33. Patient engagement in research can support more relevant research through better alignment with patients’ and clinicians’ real-world needs and concerns 34, 35.
There are known barriers to patient recruitment, involvement, and engagement in research 35. Additionally, there are known barriers to engage African Americans in research. Historically, the African American community distrusts healthcare, specifically regarding research 27. Additional barriers include compensation, education disadvantage, lack of interest, inability to have study partner, and lack of transportation 36.


Not One More Life Fund
Asthma disproportionally affects African Americans, Hispanics and Native Americans. Your special gift will allow us to grow focused programs in outreach, education, advocacy and research to address health disparities through our Not One More Life program.
What is Not One More Life?
In response to persistent disparities in the prevalence, morbidity and mortality rates of asthma among children, minorities and the poor, Dr. LeRoy Graham took action. He recognized that barriers existed in the urban environment that kept families who live with asthma from achieving good treatment and asthma control. Social determinants of health such as inadequate nutrition and poor outdoor and indoor air quality, coupled with limited access to care, creates an imbalance in the quality of care that some patients receive.
After losing a young man named Kellen Edwin Boldento to asthma in 2001, Dr. Graham developed a program called “Not One More Life (NOML).”

What does Not One More Life do to impact health disparities?
This is a community-based program of education, screening, counseling, referral and outcome monitoring that began small and has grown to many urban settings in the United States. This novel program brings asthma care to the heart of the community, with programs held in faith-based settings and schools. Healthcare professionals, including physicians, respiratory therapists, nurses and asthma educators, screen participants for asthma by using a validated questionnaire and spirometry. Participants that are identified as needing follow-up care are referred to a healthcare provider or specialty care and followed by a case manager.
Why are faith communities the setting for Not One More Life?
It is really very simple. Communities of faith are enduring bases of leadership in the community and foster both physical and spiritual well-being in their neighborhood. NOML screenings found that only 17% of participants had a low symptom score and normal lung function, while 38.5% had a high symptom score and abnormal lung function. The best news of NOML is that 90% of the participants reported seeing a physician after a NOML session.
There’s a lot of work to be done to improve asthma care for communities of color and NOML is a model program of bringing care to where it is needed most.
Articles on Health Disparities

Allergy & Asthma Network Applauds National Academies’ Report to Improve Health Equity
The National Academies of Science, Engineering, and Medicine recommends the federal government integrate health equity in its programs, policies and legislation.

Allergy & Asthma Network Urges Biden, Congress to Prioritize Values-Based Healthcare
Health groups are urging President Biden, Congress to put healthcare, health inequities and lower drug prices at the center of economic recovery.

Asthma, Covid-19, Questions We Need Answered: Black People Like Me Virtual Conference Series
Join us for a free virtual event to better understand and address the impact of asthma and COVID-19 in the Black community.

COVID-19 Vaccine – Treatment, Trust & Health Inequities
In this recorded webinar, speakers give us a COVID-19 vaccine update including challenges in vaccination related to trust and health inequities.

Allergy & Asthma Network Announces National Trusted Messengers Project to Address Health Inequities
The Trusted Messengers project will address inequities in health exposed by the COVID-19 pandemic and improve long-term health outcomes in communities of color.

Allergy & Asthma Network to Host COVID-19, Asthma and COPD Screenings at Atlanta Churches
September 2020 – Allergy & Asthma Network Will Promote Health Equity by Hosting Free COVID-19, Asthma & COPD Screenings at Atlanta Churches.

Disparities in Food Allergy – Racial, Ethnic & Socioeconomic Considerations
Join us on Sept. 24 when Dr. Ruchi Gupta will discuss racial/ethnic differences in food allergy prevalence, outcomes, care and management.

A Tale of Two Asthma Patients: How Social and Economic Factors Impact Asthma
Learn through the stories of two young men with asthma how social and economic factors influence health and access to medical care.

Allergy & Asthma Network Secures PCORI Engagement Award, CDC Grant to Reduce COVID-19 and Asthma Disparities
Allergy & Asthma Network is working to address COVID-19 and asthma health disparities through a PCORI Engagement Award and CDC Grant.

‘Not One More Life’ Makes an Impact on Asthma Disparities in Communities of Color
Learn about Not One More Life, a program of the Allergy & Asthma Network that brings asthma screenings and education to vulnerable populations in the U.S.

Black Individuals at Higher Risk for Contracting COVID-19 – New Research
Learn more about a new study showing that Black individuals were twice as likely as White individuals to test positive for COVID-19.

Allergy & Asthma Network Advocates for People Living with Health Disparities
Learn about our efforts that bring an end to racial disparities affecting people with asthma, allergies and related conditions.
Meet Dr. LeRoy Graham
An innovator leader in the Health Disparity cause
How does Allergy & Asthma Network address health disparities?
Allergy & Asthma Network is committed to ending racial, ethnic and socioeconomic health disparities so everyone who lives with asthma, allergies and other respiratory conditions has the opportunity to achieve their full health potential. We do this through our four central mission areas: outreach, education, advocacy and research.

Outreach
We host a series of COVID-19, asthma and COPD screenings at churches in African American communities around the country. The screenings are part of our Not One More Life Trusted Messengers program. We also work with community leaders and health advocates to correct health disparities. We do this by expanding healthcare access through digital innovation.

Education
We share news, information, research, infographics and patient stories on our media platforms. These include our website, social media, e-newsletter and print publications. We host webinars on the impact of COVID-19, asthma and allergies on African Americans, Hispanic/Latinos and Native Americans.

Advocacy
We support the passage of bills that create greater access to quality healthcare for all. We advocate for innovative treatments and a safe environment to live, work and play. We work with federal, state and local officials to pass legislation. Our recent successes include stock albuterol and epinephrine in schools and public places. We also work to reduce harmful air pollution and ensure access to safe, affordable medications.

Research
We work to encourage greater participation in research. In 2021, we are hosting a series of virtual conferences with African American asthma patients, doctors, faith-based leaders and other key stakeholders. The intent is to better engage and involve African Americans in research and improve health outcomes.
References
- https://www.healthypeople.gov/2020/about/foundation-health-measures/Disparities
- https://www.ncbi.nlm.nih.gov/books/NBK425853/
- https://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-of-health
- https://www.kff.org/disparities-policy/issue-brief/beyond-health-care-the-role-of-social-determinants-in-promoting-health-and-health-equity/
- https://minorityhealth.hhs.gov/omh/browse.aspx?lvl=3&lvlid=61
- https://www.cdc.gov/nchs/products/databriefs/db289.htm
- https://www.cdc.gov/obesity/data/adult.html
- https://www.cdc.gov/asthma/asthmadata/adult_prevalence_race.html
- https://www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf
- https://www.cdc.gov/mmwr/volumes/69/wr/pdfs/mm6915e3-H.pdf
- https://coronavirus.jhu.edu/data/racial-data-transparency
- https://www.feedingamerica.org/sites/default/files/research/map-the-meal-gap/2015/2015-mapthemealgap-exec-summary.pdf
- https://www.feedingamerica.org/hunger-in-america/african-american
- https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-us/key-statistics-graphics.aspx#householdtype
- https://ajph.aphapublications.org/doi/full/10.2105/AJPH.2017.304297
- https://www.jchs.harvard.edu/ARH_2017_cost_burdens_by_race
- https://files.hudexchange.info/resources/documents/2019-AHAR-Part-1.pdf
- https://minorityhealth.hhs.gov/omh/browse.aspx?lvl=3&lvlid=64
- https://minorityhealth.hhs.gov/omh/browse.aspx?lvl=4&lvlid=60
- https://www.pewresearch.org/hispanic/2016/04/20/the-nations-latino-population-is-defined-by-its-youth/
- https://minorityhealth.hhs.gov/omh/browse.aspx?lvl=3&lvlid=62
- https://minorityhealth.hhs.gov/omh/browse.aspx?lvl=4&lvlid=34
- https://www.cdc.gov/vitalsigns/aian-diabetes/index.html
- http://www.nativepartnership.org/site/DocServer/2017-PWNA-NPRA-Food-Insecurity-Project-Grow.pdf?docID=7106
- https://www.cnn.com/2020/05/18/us/navajo-nation-infection-rate-trnd/index.html
- https://www.cdc.gov/mmwr/volumes/69/wr/pdfs/mm6915e3-H.pdf
- https://www.ncbi.nlm.nih.gov/pubmed/19175244
- https://www.cdc.gov/coronavirus/2019-ncov/covid-data/images/us-mortality-graph-animated-06032020.jpg
- https://covidtracking.com/race/dashboard
- https://www.hrsa.gov/about/organization/bureaus/ohe/health-literacy/index.html
- https://www.aafp.org/news/blogs/leadervoices/entry/20181204lv-clinicaltrials.html
- https://www.atsjournals.org/doi/pdf/10.1164/rccm.201410-1944PP
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3938901/
- https://ascpt.onlinelibrary.wiley.com/doi/pdf/10.1111/cts.12285
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3938901/
- https://journals.sagepub.com/doi/full/10.1177/2168479017720247
{kind=link}